Thoracoscopic Lung biopsy
Basics of Lung anatomy:

Thoracoscopic Lung biopsy
Basics of Lung anatomy:
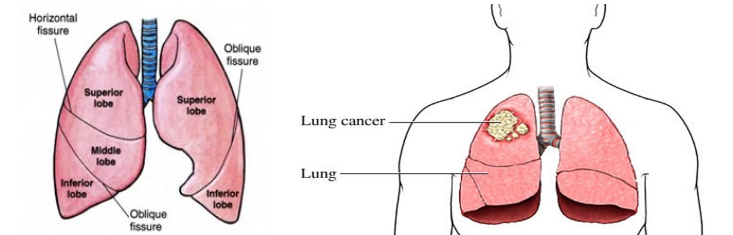
Lungs are the breathing apparatus of the human body. They have many functions but are mostly known for breathing. The other functions of lungs include filtering particulate matter from the air and charging the immune system of the body and to work with the heart in synchrony.
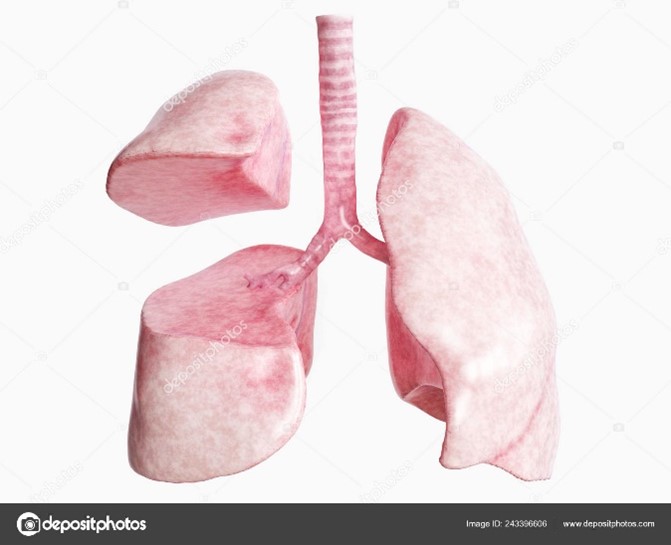
There are two lungs. The right lung has three divisions and the left lung has two divisions. The individual divisions are known as lobes. Each lobe has further subdivisions which are not visible from the outside that are known as segments.
The Trachea is a breathing pipe which is also known as the main airway. Airway (blue coloured pipe) is connected to both lungs as shown in the diagram. It has two main divisions which are right and left. Both sides have further subdivisions for different segments of lung.
Each lobe is connected to its own division of airway, blood vessels routing deoxygenated blood into lungs and blood vessels routing oxygenated blood outside of the lung.
What is a lung biopsy?
Lung biopsy is obtaining a small tissue of lung to assess it microscopically to make a diagnosis of lung conditions. Tissue can also be assessed for growth of rare bacteria causing lung conditions
How is lung biopsy obtained ?
There are two standard methods.
Thoracoscopic lung biopsy
Thoracoscopic / VATS lung biopsy
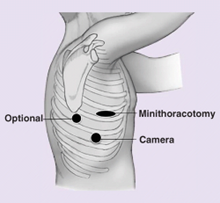
The thoracoscopic approach utilizes a small incision (1-2 cm) on the chest wall without spreading the ribs. The operation is facilitated by the introduction of a telescope in the chest cavity via a small 1 cm incision. There are many advantages of these specialised methods that include : cosmetic scar, minimal injury to ribs, chest wall muscles and nerves, and speedy recovery.
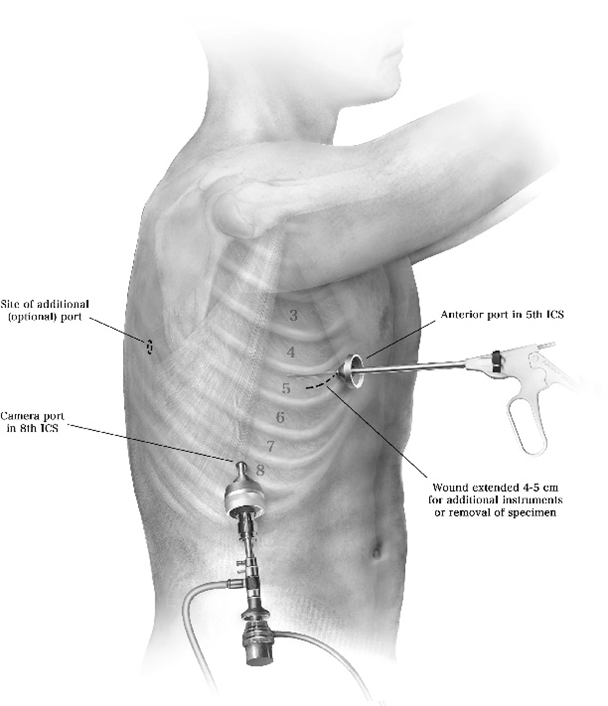
Figure: Thoracoscopic lung biopsy
VATS lung biopsy is done under general anaesthesia meaning that the patient is fully asleep and does not feel any pain/sensation or be aware of the operation. The anaesthetist uses a specialised technique that allows for patients to breathe via the lung that is not being operated on. Urinary catheterization is not generally used. However, if patients fail to pass urine after surgery then catheterization may be necessary.
The duration of surgery is about 20-30 mins for the surgical part. Time for delivery of anaesthesia and preparation for surgery adds another 30 mins to the surgery. Patients are woken up straight after completion of surgery. There is a drain inserted on the side of the operation. The purpose of the drain is to remove any fluid or blood that may have collected during surgery and also to remove any fluid or air after surgery.

Portable chest drain system displaying air leak and fluid drainage volume.
Surgeons use surgical staplers to cut a little piece of tissue from the lung. The stapler uses 3 rows of fine titanium staples to seal the division of lungs. When patients start to breathe from the side of the operated lungs, they start to breathe air on that side. Some of the air can leak from the holes created by the row of staples. Majority of them seal straight away but sometimes it can take longer for the tiny holes to seal. To evacuate the air leaking from tiny holes, a little drain is placed in the operated side of your chest. So, one of the most important purposes of the drain is to remove air that may leak from the staples hole after lung resection surgery. Most surgeons will remove drains in 6-24 hrs after air leak has stopped.
After surgery the patient stays in the recovery room until the anaesthetic wears off. After that the patient is transferred to the ward. Typically, the stay after surgery is expected to be between 1-2 days. It takes about 2-3 weeks to become independent and get back to work. You should not drive for 2 weeks.

For the first two days, the most important thing that patients have to deal with is pain from the operation and drains. Pain control methods include oral tablets, intravenous infusions and infusions around the spinal cord. Depending on the patient’s background history the anaesthetist decides the pain control method. Some of the methods include a patient initiated analgesia regimen which may include an infusion that patient can control or on demand tablets for pain control.
While recuperating in the ward patients are visited by physiotherapists. The patients are encouraged to participate in regular physiotherapy and mobilization. Apart from drains, patients are connected to an infusion system to control pain. It is quite cumbersome to move in and out of bed while drains and infusions are connected. Nursing staff will provide you with assistance. The patient can also call for the staff if they want to move out of bed. Accidental disconnection of the drain system or infusion can cause complications and it’s better avoided.
Your drain site has a dressing on it. Occasionally it can stain with blood-stained fluid. You need to inform your staff. This is due to fluid collected in the chest leaking around the drainage pipe. To experience this is uncomfortable but this is not a complication. Nurses may need to change the dressing frequently and will discuss with Dr Joshi. Dr Joshi will advise on a further course of action.
Dr Joshi will visit you on alternate days and his practice nurse will also visit you while you are in the ward. The staff stays in regular communication with Dr Joshi about your progress. Your recuperation plan is guided by Dr Joshi. He will discuss with you regarding your discharge plan. Prior to you being discharged you will be given discharge instruction that includes:
It is not uncommon to cough blood-stained phlegm for a few days after surgery. This is due to surgical handling of the airways during surgery. You should inform your surgeon but generally it subsides on its own.
Some lung conditions can worsen with the stress of surgery and general anaesthesia. It may require admission to ICU and use of a respirator. This complication is uncommon but worth being aware of.
You may experience a fever in the first 48 hours and your blood counts are expected to rise. This is not a sign of infection. However, if fever persists then some additional tests may be carried out and treatment will be commenced if infection is suspected.
Nausea, vomiting and constipation are common side effects of pain medications and anaesthetic medications. Your staff will titrate the dose of pain medications for you to get optimum pain relief and to minimize side effects of pain medications. Pain does not completely disappear but the goal is to keep pain within the limit of tolerance and allow for carrying out exercise and physiotherapy.
Infection of wounds, chest cavity and airway stump (divided end of airway) can occur however, but is very uncommon unless specific risk factors are present in patient (e.g. Patients on steroids, immunosuppressants, Diabetes, advanced cancer etc)
Life threatening complications are very rare but worth noting. Heart attacks can occur in patients with risk factors. Major bleeding can occur during surgery which may require converting keyhole surgery to open surgery to be able to control bleeding. Patients who have cancers are at risk of developing blood clots in the legs which have a risk of migrating to the heart. Patients are given injections of weak blood thinner to prevent the occurrence of clots in legs.
One of the important long term side effects to note is nerve pain. With VATS surgery, the incidence of nerve pain is less likely, however it can occur. Nerves underneath each rib are sensitive and delicate and can occasionally be damaged while removing a lung specimen. This will manifest as numbness over the front of the chest or breast. Women may feel heaviness in their breasts. These side effects are likely to improve over a period of time. Some patients may require painkillers.
The role of a surgeon in treating your lung condition is to help your specialist make a diagnosis. The surgeon does that by obtaining lung tissue with VATS lung biopsy. Dr Joshi does not actively treat your lung condition. The results of your biopsy are reviewed by your specialist and may be presented in a specialist meeting. Your respiratory physician takes over your care after Dr Joshi has performed a biopsy and you are discharged from hospital. The further treatment will depend on your diagnosis. Dr Joshi does not organise follow up routinely as the incisions are small and can be easily managed by your GP. If you want to see Dr Joshi for a follow up then you need to contact his rooms to make an appointment.